Dissection Diary Day 7: You Are A Miracle
The Organs

Every day of this dissection journey has been sacred, but today was like a very special day at church.
A holy day.
Before each lab session Gil reads from his book of poetry and today a classmate opened to a page and he first read the poem that he said was actually a song and then another classmate asked him to sing it.
It was a magical moment which extended into a beautiful guided meditation and more spontaneous singing!
Today was extra special because we opened the veil to the organs.
We stepped into the caves.
We looked behind the curtain.
We opened the hood.
And what lies within was extraordinary.
Jaw dropping magnificence.
Perfect choreography.
Each organ dances and moves in a certain way.
Differential movement.
The ability for different directions of movement to take place while saying in relationship with one another.
In the musculoskeletal system differential movement is achieved with the spider web like peri-fascia, but in the organs differential movement is achieved by sliding serous fluid between the layers of peritoneum, plural, and pericardium.
Every one playing its perfect role in the digestion, respiration, and circulation performance.
The number of things that are happening in your body right now for you to be sitting at your device reading this is astonishing.
Just think about the biochemical reactions that are taking place in each tissue.
Then think about the bioelectrical activity in the nerve signals.
Then think about the biomechanical coordination of every movement.
You could spend lifetimes learning about what we *think* the body is doing in order to sustain life… and barely scratch the surface of grokking every function and how they all coordinate together.
And as they allegedly say to medical students on the first day of class:
"Half of what you'll learn in medical school will be wrong, and we don't know which half"
It’s humbling to stand before the organs and witness how the Grand Intelligence arranged things.
The digestive tube from mouth to rectum that allows for the tissues to receive nourishment.
Completely contained in the digestive tube food goes through many transformations from entrance to exit.
You take a bite of food and usually don’t think much about it, but you just gave your body a job of trillions of electrical, chemical, and motor actions in order for it to be processed.
TRILLIONS.
And your body does it automatically.
Gil describes the organs as “a bag of jolly kittens” or “a snuggly cave of baby bears”.

After we cut through the veil posterior rectus sheath we got to see what he means.
Every abdominal organ is tucked in its spot, there are no gaps, the space is filled entirely.
First we just look at how things are arranged in situ because like we talked about before what you see in the anatomy books is not always what you see in the bodies.
The first body we explored was the largest of the 3 and she had the most ample greater omentum.
The greater omentum is a double layered extension of the peritoneum woven with adipose to create what looks like a skirt or blanket around the abdominal organs.
We chatted about the function of the omentum and Gil called it a Roomba because it goes to areas of inflammation and works as part of the “immune system”.
From the GNM perspective the peritoneum is derived from the Old Mesodermal embryological germ layer, is controlled by the cerebellum, and responds to a conflict of an Attack Against the Abdomen
This can be a literal attack like a kick or a stab during fight, it could be threatening words, or it could be a fear of attack like fear of a surgery, or feeling attacked by being given an abdominal diagnosis, even intense pain in the abdomen (intestinal, menstrual, pain during sex) could be experienced as an attack conflict.
There is cellular increase during the conflict to thicken the peritoneum during the active conflict to better protect you from the threat.
When the conflict is resolved, the extra tissue that proliferated during the conflict is removed with bacteria and you experience night sweats and some pain. (If you are also running the KCT program while in healing with the peritoneum or greater omentum this causes the condition known as ascites.)
The greater omentum has the “ugly belly conflict” which is an acute distress related to the abdomen.
During the active conflict there is cellular increase to enhance the secretion of serous fluids to improve the motility of the omentum which allows this intelligent abdominal blanket to move to areas that are inflamed.
Dr. Hamer said that if an appendix has be perforated the omentum will slide over there and seal off the area to prevent leakage.
Gil mentioned during class that you will find the omentum in different areas on different bodies which makes sense that this intelligent protective cloth goes wherever it is needed.
After examining the greater omentum we found the lesser omentum coming off the small curvature of the stomach and also palpated the epiploic foramen of the omental bursa.
Then we “ran the bowel” which is where you go inch by inch through the intestines to look for adhesions.
We also held the “bouquet” by gathering up the small intestines and passing them from person to person.

We saw the muscular uterus sitting in the pelvic bowl with the arms of the fallopian tubes and their fimbriae fingers reaching out to the ovaries.
When we observed how the uterus was positioned in the first body her right side fallopian tube was extended similar to what you’d see in a typical diagram, but her left side was kinked and pushed up closer to the abdominal wall.
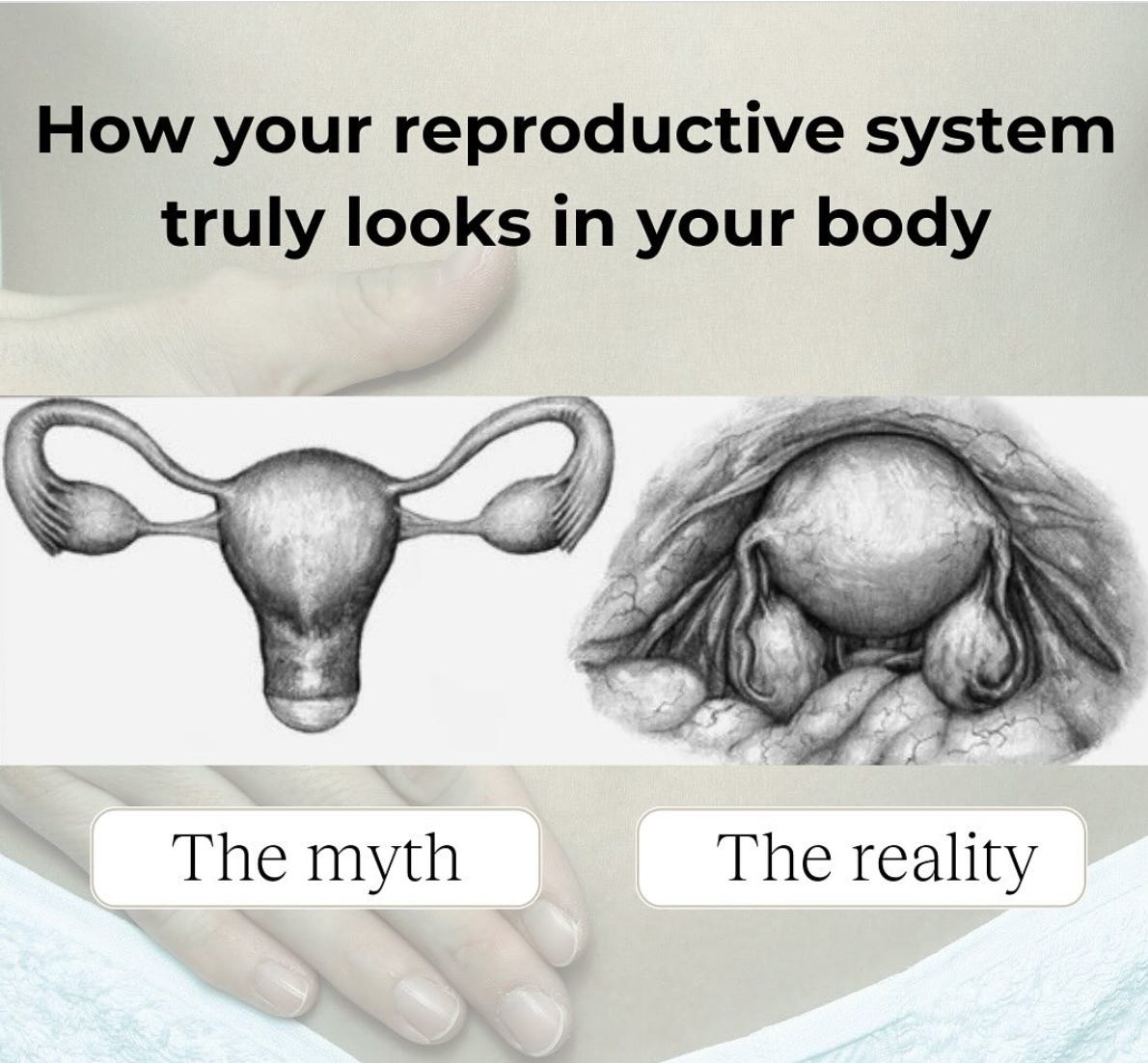
This meme recently went around on the inter webs and actually neither of these are likely true!
Your uterus and its placement is unique to your structure, alignment, and adaptations you’ve experienced.
On the 2nd body we explored, her uterus looked more like the picture, but her intestines looked nothing like what you see in the pictures!
Her entire small bowel was tucked into her deep pelvis and her transverse colon was where you’d expect to see the sigmoid.
It was such a marvel to unfold the innards to see the particular placement that was needed for this person as well as to see the adaptations and interventions that have taken place.
The first body had a gall bladder full of rocky clumps, the second body we could not find a gall bladder, and the 3rd had half of her liver missing as well as the gallbladder.
The 3rd body had many adaptations and interventions.
When we removed her posterior rectus sheath there were adhesions to the tissues underneath.
The liver was not under the right ribs as you’d expect, rather it was midline and half its normal size!
The small intestines were where the liver usually resides.
Intestinal adhesions to the abdominal wall and to each other.
A segment of small intestines removed and reconnected.
The greater omentum was a thin layer of lace instead of being a thick protective blanket.
The uterus was gone.
A deeply embedded wire was suspending the vagina.
There were diverticuliti on the rectum.
Each change tells the story of a life that was lived.
Each intervention was an attempt to fix her body and save her life.
We don’t get much information about the bodies, but her records say she was 64 years old and first had breast cancer followed by several “metastases” over 7 years.
I wonder how she felt as she was going through this.
I wonder what was happening in her life in her mid to late 50s.
I wonder what the doctors told her about what was going on.
Was she fearful or peaceful about what was happening her body?
Did she feel like a victim of bad genes or did she recognize how her body was adapting to her specific life circumstances?
I’m grateful for the gift of examining her body and to see the footprints of her experiences.
It inspires me anew to share with women and men the story of Dr. Hamer and the story of how their tissues adapt to biological conflict shocks.
On Sunday after our trip to Pikes’s Peak we spent some time in downtown Manitou and a local GNM Instagram friend came by to hang out.
We chatted over guacamole about her own breast adaptation and how she navigated it with the knowledge of the 5 Biological Laws.
She knows that if she went the traditional route she would have lost her breast like our dear donor on the table.
We talked about my Youtube video with Patty who also had a breast adaptation and navigated it without fear or intervention.
What a gift it is to know and share this wisdom.
The future of healthcare is fearless.
<3